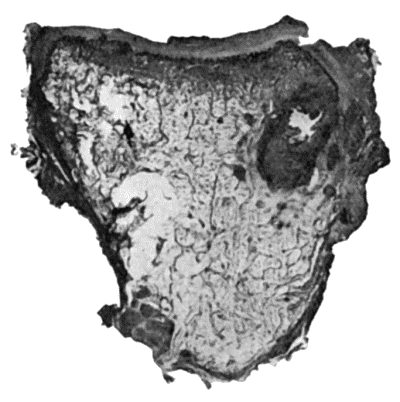
Fig. 124.—Tuberculous Osteomyelitis of Os Magnum, excised from a boy æt. 8. Note well-defined caseous focus, with several minute foci in surrounding marrow.
The tuberculous diseases of bone result from infection of the marrow or periosteum by tubercle bacilli conveyed through the arteries; it is exceedingly rare for tubercle to appear in bone as a primary infection, the bacilli being usually derived from some pre-existing focus in the bronchial glands or elsewhere. According to the observations of John Fraser, 60 per cent. of the cases of bone and joint tubercle in children are due to the bovine bacillus, 37 per cent. to the human variety, and in 3 per cent. both types are present.
Tuberculous disease in bone is characterised by its insidious onset and slow progress, and by the frequency with which it is associated with disease of the adjacent joint.
Periosteal tuberculosis is met with in the ribs, sternum, vertebral column, skull, and less frequently in the long bones of the limbs. It may originate in the periosteum, or may spread thence from the marrow, or from synovial membrane.
In superficial bones, such as the sternum, the formation of tuberculous granulation tissue in the deeper layer of the periosteum, and its subsequent caseation and liquefaction, is attended by the insidious development of a doughy swelling, which is not as a rule painful, although tender on pressure. While the swelling often remains quiescent for some time, it tends to increase in size, to become boggy or fluctuating, and to assume the characters of a cold abscess. The pus perforates the fibrous layer of the periosteum, invading and infecting the overlying soft parts, its spread being influenced by the anatomical arrangement of the tissues. The size of the abscess affords no indication of the extent of the bone lesion from which it originates. As the abscess reaches the surface, the skin becomes of a dusky red or livid colour, is gradually thinned out, and finally sloughs, forming a sinus. A probe passed into the sinus strikes carious bone. Small sequestra may be found embedded in the granulation tissue. The sinus persists as long as any active tubercle remains in the tissues, and is apt to form an avenue for pyogenic infection.
In deeply seated bones, such as the upper end of the femur, the formation of a cold abscess in the soft parts is often the first evidence of the disease.
Diagnosis.—Before the stage of cold abscess is reached, the localised swelling is to be differentiated from a gumma, from chronic forms of staphylococcal osteomyelitis, from enlarged bursa or ganglion, from sub-periosteal lipoma, and from sarcoma. Most difficulty is met with in relation to periosteal sarcoma, which must be differentiated either by the X-ray appearances or by an exploratory incision.
X-ray appearances in periosteal tubercle: the surface of the cortical bone in the area of disease is roughened and irregular by erosion, and in the vicinity there may be a deposit of new bone on the surface, particularly if a sinus is present and mixed infection has occurred; in syphilis the shadow of the bone is denser as a result of sclerosis, and there is usually more new bone on the surface—hyperostosis; in periosteal sarcoma there is greater erosion and consequently greater irregularity in the contour of the cortical bone, and frequently there is evidence of formation of bone in the form of characteristic spicules projecting from the surface at a right angle.
The early recognition of periosteal lesions in the articular ends of bones is of importance, as the disease, if left to itself, is liable to spread to the adjacent joint.
The treatment is that of tuberculous lesions in general; if conservative measures fail, the choice lies between the injection of iodoform, and removal of the infected tissues with the sharp spoon. In the ribs it is more satisfactory to remove the diseased portion of bone along with the wall of the associated abscess or sinus. If all the tubercle has been removed and there is no pyogenic infection, the wound is stitched up with the object of obtaining primary union; otherwise it is treated by the open method.
Fig. 124.—Tuberculous Osteomyelitis of Os Magnum, excised from a boy æt. 8. Note well-defined caseous focus, with several minute foci in surrounding marrow.
Tuberculous Osteomyelitis.—Tuberculous lesions in the marrow occur as isolated or as multiple foci of granulation tissue, which replace the marrow and erode the trabeculæ of bone in the vicinity (Fig. 124). The individual focus varies in size from a pea to a walnut. The changes that ensue resemble in character those in other tissues, and the extent of the destruction varies according to the way in which the tubercle bacillus and the marrow interact upon one another. The granulation tissue may undergo caseation and liquefaction, or may become encapsulated by fibrous tissue—“encysted tubercle.”
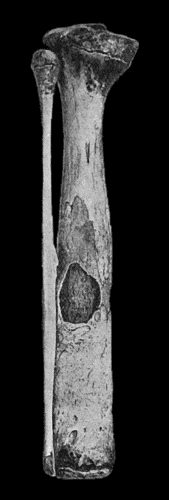
Fig. 125.—Tuberculous Disease of Child's Tibia, showing sequestrum in medullary cavity, and increase in girth from excess of new bone.
Sometimes the tuberculous granulation tissue spreads in the marrow, assuming the characters of a diffuse infiltration—diffuse tuberculous osteomyelitis. The trabecular framework of the bone undergoes erosion and absorption—rarefying ostitis—and either disappears altogether or only irregular fragments or sequestra of microscopic dimensions remain in the area affected. Less frequently the trabecular framework is added to by the formation of new bone, resulting in a remarkable degree of sclerosis, and if, following upon this, there is caseation of the tubercle and death of the affected portion of bone, there results a sequestrum often of considerable size and characteristic shape, which, because of the sclerosis and surrounding endarteritis, is exceedingly slow in separating. When the sequestrum involves an articular surface it is often wedge-shaped; in other situations it is rounded or truncated and lies in the long axis of the medullary canal (Fig. 125). Finally, the sequestrum lies loose in a cavity lined by tuberculous granulation tissue, and is readily identified in a radiogram. This type of sclerosis preceding death of the bone is highly characteristic of tuberculosis.
Clinical Features.—As a rule, it is only in superficially placed bones, such as the tibia, ulna, clavicle, mandible, or phalanges, that tuberculous disease in the marrow gives rise to signs sufficiently definite to allow of its clinical recognition. In the vertebræ, or in the bones of deeply seated joints, such as the hip or shoulder, the existence of tuberculous lesions in the marrow can only be inferred from indirect signs—such, for example, as rigidity and curvature in the case of the spine, or from the symptoms of grave and persistent joint-disease in the case of the hip or shoulder.
With few exceptions, tuberculous disease in the interior of a bone does not reveal its presence until by extension it reaches one or other of the surfaces of the bone. In the shaft of a long bone its eruption on the periosteal surface is usually followed by the formation of a cold abscess in the overlying soft parts. When situated in the articular ends of bones, the disease more often erupts in relation to the reflection of the synovial membrane or directly on the articular surface—in either case giving rise to disease of the joint (Fig. 156).
Diffuse Tuberculous Osteomyelitis in the shaft of a long bone is comparatively rare, and has been observed chiefly in the tibia and the ulna in children (Fig. 126). It commences at the growing extremity of the diaphysis, and spreads along the medulla to a variable extent; it is attended by the formation of vascular and porous bone on the surface, which causes thickening of the diaphysis; this is most marked at the ossifying junction and tapers off along the shaft. The infection not only spreads along the medulla, but it invades the spongy bone surrounding this, and then the cortical bone, and is only prevented from reaching the soft parts by the new bone formed by the periosteum. The bone is replaced by granulation tissue, and disappears, or part of it may become sclerosed and in time form a sequestrum. In the macerated specimen, the sequestrum appears small in proportion to the large cavity in which it lies. All these changes are revealed in a good skiagram, which not only confirms the diagnosis, but, in many instances, demonstrates the extent of the disease, the presence or absence of a sequestrum, and the amount of new bone on the surface. Finally the periosteum gives way, and an abscess forms in the soft parts; and if left to itself ruptures externally, leaving a sinus. The most satisfactory treatment is to resect sub-periosteally the diseased portion of the diaphysis.
In cancellous bones, such as those of the tarsus, there is a similar caseous infiltration in the marrow, and this may be attended with the formation of a sequestrum either in the interior of the bone or involving its outer shell, as shown in Fig. 127. The situation and extent of the disease are shown in X-ray photographs. After the tuberculous granulation tissue erupts through the cortex of the bone, it gives rise to a cold abscess or infects adjacent joints or tendon sheaths.
If an exact diagnosis is made at an early stage of the disease—and this is often possible with the aid of X-rays—the affected bone is excised sub-periosteally or its interior is cleared out with the sharp spoon and gouge, the latter procedure being preferred in the case of the calcaneus to conserve the stability of the heel. When several bones and joints are simultaneously affected, and there are sinuses with mixed infection, amputation is usually indicated, especially in adults.

Fig. 127.—Advanced Tuberculous Disease in region of Ankle. The ankle-joint is ankylosed, and there is a large sequestrum in the calcaneus.
(Specimen in Anatomical Museum, University of Edinburgh.)
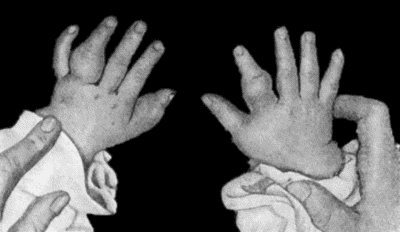
Tuberculous dactylitis is the name applied to a diffuse form of the disease as it affects the phalanges, metacarpal or metatarsal bones. The lesion presents, on a small scale, all the anatomical changes that have been described as occurring in the medulla of the tibia or ulna, and they are easily followed in skiagrams. A periosteal type of dactylitis is also met with.
The clinical features are those of a spindle-shaped swelling of a finger or toe, indolent, painless, and interfering but little with the function of the digit. Recovery may eventually occur without suppuration, but it is common to have the formation of a cold abscess, which bursts and forms one or more sinuses. It may be difficult to differentiate tuberculous dactylitis from the enlargement of the phalanges in inherited syphilis (syphilitic dactylitis), especially when the tuberculous lesion occurs in a child who is the subject of inherited syphilis.
In the syphilitic lesion, skiagrams usually show a more abundant formation of new bone, but in many cases the doubt is only cleared up by observing the results of the tuberculin test or the effects of anti-syphilitic treatment.
Sarcoma of a phalanx or metacarpal bone may closely resemble a dactylitis both clinically and in skiagrams, but it is rare.
Treatment.—Recovery under conservative measures is not uncommon, and the functional results are usually better than those following upon operative treatment, although in either case the affected finger is liable to be dwarfed (Fig. 129). The finger should be immobilised in a splint, and a Bier's bandage applied to the upper arm. Operative interference is indicated if a cold abscess develops, if there is a persistent sinus, or if a sequestrum has formed, a point upon which information is obtained by examination with the X-rays. When a toe is affected, amputation is the best treatment, but in the case of a finger it is rarely called for. In the case of a metacarpal or metatarsal bone, sub-periosteal resection is the procedure of choice, saving the articular ends if possible.