Fig. 6.—Passive Hyperæmia of Hand and Forearm induced by Bier's Bandage.
Inflammation may be defined as the series of vital changes that occurs in the tissues in response to irritation. These changes represent the reaction of the tissue elements to the irritant, and constitute the attempt made by nature to arrest or to limit its injurious effects, and to repair the damage done by it.
The phenomena which characterise the inflammatory reaction can be induced by any form of irritation—such, for example, as mechanical injury, the application of heat or of chemical substances, or the action of pathogenic bacteria and their toxins—and they are essentially similar in kind whatever the irritant may be. The extent to which the process may go, however, and its effects on the part implicated and on the system as a whole, vary with different irritants and with the intensity and duration of their action. A mechanical, a thermal, or a chemical irritant, acting alone, induces a degree of reaction directly proportionate to its physical properties, and so long as it does not completely destroy the vitality of the part involved, the changes in the tissues are chiefly directed towards repairing the damage done to the part, and the inflammatory reaction is not only compatible with the occurrence of ideal repair, but may be looked upon as an integral step in the reparative process.
The irritation caused by infection with bacteria, on the other hand, is cumulative, as the organisms not only multiply in the tissues, but in addition produce chemical poisons (toxins) which aggravate the irritative effects. The resulting reaction is correspondingly progressive, and has as its primary object the expulsion of the irritant and the limitation of its action. If the natural protective effort is successful, the resulting tissue changes subserve the process of repair, but if the bacteria gain the upper hand in the struggle, the inflammatory reaction becomes more intense, certain of the tissue elements succumb, and the process for the time being is a destructive one. During the stage of bacterial inflammation, reparative processes are in abeyance, and it is only after the inflammation has been allayed, either by natural means or by the aid of the surgeon, that repair takes place.
In applying the antiseptic principle to the treatment of wounds, our main object is to exclude or to eliminate the bacterial factor, and so to prevent the inflammatory reaction going beyond the stage in which it is protective, and just in proportion as we succeed in attaining this object, do we favour the occurrence of ideal repair.
Sequence of Changes in Bacterial Inflammation.—As the form of inflammation with which we are most concerned is that due to the action of bacteria, in describing the process by which the protective influence of the inflammatory reaction is brought into play, we shall assume the presence of a bacterial irritant.
The introduction of a colony of micro-organisms is quickly followed by an accumulation of wandering cells, and proliferation of connective-tissue cells in the tissues at the site of infection. The various cells are attracted to the bacteria by a peculiar chemical or biological power known as chemotaxis, which seems to result from variations in the surface tension of different varieties of cells, probably caused by some substance produced by the micro-organisms. Changes in the blood vessels then ensue, the arteries becoming dilated and the rate of the current in them being for a time increased—active hyperæmia. Soon, however, the rate of the blood flow becomes slower than normal, and in course of time the current may cease (stasis), and the blood in the vessels may even coagulate (thrombosis). Coincidently with these changes in the vessels, the leucocytes in the blood of the inflamed part rapidly increase in number, and they become viscous and adhere to the vessel wall, where they may accumulate in large numbers. In course of time the leucocytes pass through the vessel wall—emigration of leucocytes—and move towards the seat of infection, giving rise to a marked degree of local leucocytosis. Through the openings by which the leucocytes have escaped from the vessels, red corpuscles may be passively extruded—diapedesis of red corpuscles. These processes are accompanied by changes in the endothelium of the vessel walls, which result in an increased formation of lymph, which transudes into the meshes of the connective tissue giving rise to an inflammatory œdema, or, if the inflammation is on a free surface, forming an inflammatory exudate. The quantity and characters of this exudate vary in different parts of the body, and according to the nature, virulence, and location of the organisms causing the inflammation. Thus it may be serous, as in some forms of synovitis; sero-fibrinous, as in certain varieties of peritonitis, the fibrin tending to limit the spread of the inflammation by forming adhesions; croupous, when it coagulates on a free surface and forms a false membrane, as in diphtheria; hæmorrhagic when mixed with blood; or purulent, when suppuration has occurred. The protective effects of the inflammatory reaction depend for the most part upon the transudation of lymph and the emigration of leucocytes. The lymph contains the opsonins which act on the bacteria and render them less able to resist the attack of the phagocytes, as well as the various protective antibodies which neutralise the toxins. The polymorph leucocytes are the principal agents in the process of phagocytosis (p. 22), and together with the other forms of phagocytes they ingest and destroy the bacteria.
If the attempt to repel the invading organisms is successful, the irritant effects are overcome, the inflammation is arrested, and resolution is said to take place.
Certain of the vascular and cellular changes are now utilised to restore the condition to the normal, and repair ensues after the manner already described. In certain situations, notably in tendon sheaths, in the cavities of joints, and in the interior of serous cavities, for example the pleura and peritoneum, the restoration to the normal is not perfect, adhesions forming between the opposing surfaces.
If, however, the reaction induced by the infection is insufficient to check the growth and spread of the organisms, or to inhibit their toxin production, local necrosis of tissue may take place, either in the form of suppuration or of gangrene, or the toxins absorbed into the circulation may produce blood-poisoning, which may even prove fatal.
Clinical Aspects of Inflammation.—It must clearly be understood that inflammation is not to be looked upon as a disease in itself, but rather as an evidence of some infective process going on in the tissues in which it occurs, and of an effort on the part of these tissues to overcome the invading organisms and their products. The chief danger to the patient lies, not in the reactive changes that constitute the inflammatory process, but in the fact that he is liable to be poisoned by the toxins of the bacteria at work in the inflamed area.
Since the days of Celsus (first century A.D.), heat, redness, swelling, and pain have been recognised as cardinal signs of inflammation, and to these may be added, interference with function in the inflamed part, and general constitutional disturbance. Variations in these signs and symptoms depend upon the acuteness of the condition, the nature of the causative organism and of the tissue attacked, the situation of the part in relation to the surface, and other factors.
The heat of the inflamed part is to be attributed to the increased quantity of blood present in it, and the more superficial the affected area the more readily is the local increase of temperature detected by the hand. This clinical point is best tested by placing the palm of the hand and fingers for a few seconds alternately over an uninflamed and an inflamed area, otherwise under similar conditions as to coverings and exposure. In this way even slight differences may be recognised.
Redness, similarly, is due to the increased afflux of blood to the inflamed part. The shade of colour varies with the stage of the inflammation, being lighter and brighter in the early, hyperæmic stages, and darker and duskier when the blood flow is slowed or when stasis has occurred and the oxygenation of the blood is defective. In the thrombotic stage the part may assume a purplish hue.
The swelling is partly due to the increased amount of blood in the affected part and to the accumulation of leucocytes and proliferated tissue cells, but chiefly to the exudate in the connective tissue—inflammatory œdema. The more open the structure of the tissue of the part, the greater is the amount of swelling—witness the marked degree of œdema that occurs in such parts as the scrotum or the eyelids.
Pain is a symptom seldom absent in inflammation. Tenderness—that is, pain elicited on pressure—is one of the most valuable diagnostic signs we possess, and is often present before pain is experienced by the patient. That the area of tenderness corresponds to the area of inflammation is almost an axiom of surgery. Pain and tenderness are due to the irritation of nerve filaments of the part, rendered all the more sensitive by the abnormal conditions of their blood supply. In inflammatory conditions of internal organs, for example the abdominal viscera, the pain is frequently referred to other parts, usually to an area supplied by branches from the same segment of the cord as that supplying the inflamed part.
For purposes of diagnosis, attention should be paid to the terms in which the patient describes his pain. For example, the pain caused by an inflammation of the skin is usually described as of a burning or itching character; that of inflammation in dense tissues like periosteum or bone, or in encapsuled organs, as dull, boring, or aching. When inflammation is passing on to suppuration the pain assumes a throbbing character, and as the pus reaches the surface, or “points,” as it is called, sharp, darting, or lancinating pains are experienced. Inflammation involving a nerve-trunk may cause a boring or a tingling pain; while the implication of a serous membrane such as the pleura or peritoneum gives rise to a pain of a sharp, stabbing character.
Interference with the function of the inflamed part is always present to a greater or less extent.
Constitutional Disturbances.—Under the term constitutional disturbances are included the presence of fever or elevation of temperature; certain changes in the pulse rate and the respiration; gastro-intestinal and urinary disturbances; and derangements of the central nervous system. These are all due to the absorption of toxins into the general circulation.
Temperature.—A marked rise of temperature is one of the most constant and important concomitants of acute inflammatory conditions, and the temperature chart forms a fairly reliable index of the state of the patient. The toxins interfere with the nerve-centres in the medulla that regulate the balance between the production and the loss of body heat.
Clinically the temperature is estimated by means of a self-registering thermometer placed, for from one to five minutes, in close contact with the skin in the axilla, or in the mouth. Sometimes the thermometer is inserted into the rectum, where, however, the temperature is normally ¾° F. higher than in the axilla.
In health the temperature of the body is maintained at a mean of about 98.4° F. (37° C.) by the heat-regulating mechanism. It varies from hour to hour even in health, reaching its maximum between four and eight in the evening, when it may rise to 99° F., and is at its lowest between four and six in the morning, when it may be about 97° F.
The temperature is more easily disturbed in children than in adults, and may become markedly elevated (104° or 105° F.) from comparatively slight causes; in the aged it is less liable to change, so that a rise to 103° or 104° F. is to be looked upon as indicating a high state of fever.
A sudden rise of temperature is usually associated with a feeling of chilliness down the back and in the limbs, which may be so marked that the patient shivers violently, while the skin becomes cold, pale, and shrivelled—cutis anserina. This is a nervous reaction due to a want of correspondence between the internal and the surface temperature of the body, and is known clinically as a rigor. When the temperature rises gradually the chill is usually slight and may be unobserved. Even during the cold stage, however, the internal temperature is already raised, and by the time the chill has passed off its maximum has been reached.
The pulse is always increased in frequency, and usually varies directly with the height of the temperature. Respiration is more active during the progress of an inflammation; and bronchial catarrh is common apart from any antecedent respiratory disease.
Gastro-intestinal disturbances take the form of loss of appetite, vomiting, diminished secretion of the alimentary juices, and weakening of the peristalsis of the bowel, leading to thirst, dry, furred tongue, and constipation. Diarrhœa is sometimes present. The urine is usually scanty, of high specific gravity, rich in nitrogenous substances, especially urea and uric acid, and in calcium salts, while sodium chloride is deficient. Albumin and hyaline casts may be present in cases of severe inflammation with high temperature. The significance of general leucocytosis has already been referred to.
General Principles of Treatment.—The capacity of the inflammatory reaction for dealing with bacterial infections being limited, it often becomes necessary for the surgeon to aid the natural defensive processes, as well as to counteract the local and general effects of the reaction, and to relieve symptoms.
The ideal means of helping the tissues is by removing the focus of infection, and when this can be done, as for example in a carbuncle or an anthrax pustule, the infected area may be completely excised. When the focus is not sufficiently limited to admit of this, the infected tissue may be scraped away with the sharp spoon, or destroyed by caustics or by the actual cautery. If this is inadvisable, the organisms may be attacked by strong antiseptics, such as pure carbolic acid.
Moist dressings favour the removal of bacteria by promoting the escape of the inflammatory exudate, in which they are washed out.
Artificial Hyperæmia.—When such direct means as the above are impracticable, much can be done to aid the tissues in their struggle by improving the condition of the circulation in the inflamed area, so as to ensure that a plentiful supply of fresh arterial blood reaches it. The beneficial effects of hot fomentations and poultices depend on their causing a dilatation of the vessels, and so inducing a hyperæmia in the affected area. It has been shown experimentally that repeated, short applications of moist heat (not exceeding 106° F.) are more efficacious than continuous application. It is now believed that the so-called counter-irritants—mustard, iodine, cantharides, actual cautery—act in the same way; and the method of treating erysipelas by applying a strong solution of iodine around the affected area is based on the same principle.
While these and similar methods have long been employed in the treatment of inflammatory conditions, it is only within comparatively recent years that their mode of action has been properly understood, and to August Bier belongs the credit of having put the treatment of inflammation on a scientific and rational basis. Recognising the “beneficent intention” of the inflammatory reaction, and the protective action of the leucocytosis which accompanies the hyperæmic stages of the process, Bier was led to study the effects of increasing the hyperæmia by artificial means. As a result of his observations, he has formulated a method of treatment which consists in inducing an artificial hyperæmia in the inflamed area, either by obstructing the venous return from the part (passive hyperæmia), or by stimulating the arterial flow through it (active hyperæmia).
Bier's Constricting Bandage.—To induce a passive hyperæmia in a limb, an elastic bandage is applied some distance above the inflamed area sufficiently tightly to obstruct the venous return from the distal parts without arresting in any way the inflow of arterial blood (Fig. 6). If the constricting band is correctly applied, the parts beyond become swollen and œdematous, and assume a bluish-red hue, but they retain their normal temperature, the pulse is unchanged, and there is no pain. If the part becomes blue, cold, or painful, or if any existing pain is increased, the band has been applied too tightly. The hyperæmia is kept up from twenty to twenty-two hours out of the twenty-four, and in the intervals the limb is elevated to get rid of the œdema and to empty it of impure blood, and so make room for a fresh supply of healthy blood when the bandage is re-applied. As the inflammation subsides, the period during which the band is kept on each day is diminished; but the treatment should be continued for some days after all signs of inflammation have subsided.
This method of treating acute inflammatory conditions necessitates close supervision until the correct degree of tightness of the band has been determined.
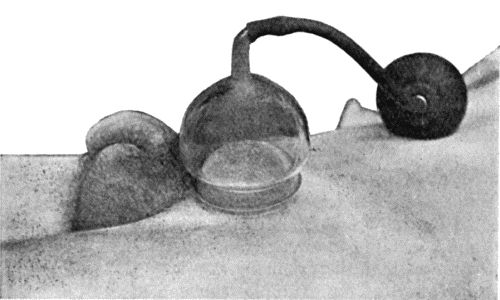
Klapp's Suction Bells.—In inflammatory conditions to which the constricting band cannot be applied, as for example an acute mastitis, a bubo in the groin, or a boil on the neck, the affected area may be rendered hyperæmic by an appropriately shaped glass bell applied over it and exhausted by means of a suction-pump, the rarefaction of the air in the bell determining a flow of blood into the tissues enclosed within it (Figs. 7 and 8). The edge of the bell is smeared with vaseline, and the suction applied for from five to ten minutes at a time, with a corresponding interval between the applications. Each sitting lasts for from half an hour to an hour, and the treatment may be carried out once or twice a day according to circumstances. This apparatus acts in the same way as the old-fashioned dry cup, and is more convenient and equally efficacious.
Active hyperæmia is induced by the local application of heat, particularly by means of hot air. It has not proved so useful in acute inflammation as passive hyperæmia, but is of great value in hastening the absorption of inflammatory products and in overcoming adhesions and stiffness in tendons and joints.
General Treatment.—The patient should be kept at rest, preferably in bed, to diminish the general tissue waste; and the diet should be restricted to fluids, such as milk, beef-tea, meat juices or gruel, and these may be rendered more easily assimilable by artificial digestion if necessary. To counteract the general effect of toxins absorbed into the circulation, specific antitoxic sera are employed in certain forms of infection, such as diphtheria, streptococcal septicæmia, and tetanus. In other forms of infection, vaccines are employed to increase the opsonic power of the blood. When such means are not available, the circulating toxins may to some extent be diluted by giving plenty of bland fluids by the mouth or normal salt solution by the rectum.
The elimination of the toxins is promoted by securing free action of the emunctories. A saline purge, such as half an ounce of sulphate of magnesium in a small quantity of water, ensures a free evacuation of the bowels. The kidneys are flushed by such diluent drinks as equal parts of milk and lime water, or milk with a dram of liquor calcis saccharatus added to each tumblerful. Barley-water and “Imperial drink,” which consists of a dram and a half of cream of tartar added to a pint of boiling water and sweetened with sugar after cooling, are also useful and non-irritating diuretics. The skin may be stimulated by Dover's powder (10 grains) or liquor ammoniæ acetatis in three-dram doses every four hours.
Various drugs administered internally, such as quinine, salol, salicylate of iron, and others, have a reputation, more or less deserved, as internal antiseptics.
Weakness of the heart, as indicated by the condition of the pulse, is treated by the use of such drugs as digitalis, strophanthus, or strychnin, according to circumstances.
Gastro-intestinal disturbances are met by ordinary medical means. Vomiting, for example, can sometimes be checked by effervescing drinks, such as citrate of caffein, or by dilute hydrocyanic acid and bismuth. In severe cases, and especially when the vomited matter resembles coffee-grounds from admixture with altered blood—the so-called post-operative hæmatemesis—the best means of arresting the vomiting is by washing out the stomach. Thirst is relieved by rectal injections of saline solution. The introduction of saline solution into the veins or by the rectum is also useful in diluting and hastening the elimination of circulating toxins.
In surgical inflammations, as a rule, nothing is gained by lowering the temperature, unless at the same time the cause is removed. When severe or prolonged pyrexia becomes a source of danger, the use of hot or cold sponging, or even the cold bath, is preferable to the administration of drugs.
Relief of Symptoms.—For the relief of pain, rest is essential. The inflamed part should be placed in a splint or other appliance which will prevent movement, and steps must be taken to reduce its functional activity as far as possible. Locally, warm and moist dressings, such as a poultice or fomentation, may be used. To make a fomentation, a piece of flannel or lint is wrung out of very hot water or antiseptic lotion and applied under a sheet of mackintosh. Fomentations should be renewed as often as they cool. An ordinary india-rubber bag filled with hot water and fixed over the fomentation, by retaining the heat, obviates the necessity of frequently changing the application. The addition of a few drops of laudanum sprinkled on the flannel has a soothing effect. Lead and opium lotion is a useful, soothing application employed as a fomentation. We prefer the application of lint soaked in a 10 per cent. aqueous or glycerine solution of ichthyol, or smeared with ichthyol ointment (1 in 3). Belladonna and glycerine, equal parts, may be used.
Dry cold obtained by means of icebags, or by Leiter's lead tubes through which a continuous stream of ice-cold water is kept flowing, is sometimes soothing to the patient, but when the vessels in the inflamed part are greatly congested its use is attended with considerable risk, as it not only contracts the arterioles supplying the part, but also diminishes the outflow of venous blood, and so may determine gangrene of tissues already devitalised.
A milder form of employing cold is by means of evaporating lotions: a thin piece of lint or gauze is applied over the inflamed part and kept constantly moist with the lotion, the dressing being left freely exposed to allow of continuous evaporation. A useful evaporating lotion is made up as follows: take of chloride of ammonium, half an ounce; rectified spirit, one ounce; and water, seven ounces.
The administration of opiates may be necessary for the relief of pain.
The accumulation of an excessive amount of inflammatory exudate may endanger the vitality of the tissues by pressing on the blood vessels to such an extent as to cause stasis, and by concentrating the local action of the toxins. Under such conditions the tension should be relieved and the exudate with its contained toxins removed by making an incision into the inflamed tissues, and applying a suction bell. When the exudate has collected in a synovial cavity, such as a joint or bursa, it may be withdrawn by means of a trocar and cannula. There are other methods of withdrawing blood and exudate from an inflamed area, for example by leeches or wet-cupping, but they are seldom employed now.
Before applying leeches the part must be thoroughly cleansed, and if the leech is slow to bite, may be smeared with cream. The leech is retained in position under an inverted wine-glass or wide test-tube till it takes hold. After it has sucked its fill it usually drops off, having withdrawn a dram or a dram and a half of blood. If it be desirable to withdraw more blood, hot fomentations should be applied to the bite. As it is sometimes necessary to employ considerable pressure to stop the bleeding, leeches should, if possible, be applied over a bone which will furnish the necessary resistance. The use of styptics may be called for.
Wet-cupping has almost entirely been superseded by the use of Klapp's suction bells.
General blood-letting consists in opening a superficial vein (venesection) and allowing from eight to ten ounces of blood to flow from it. It is seldom used in the treatment of surgical forms of inflammation.
Counter-irritants.—In deep-seated inflammations, counter-irritants are sometimes employed in the form of mustard leaves or blisters, according to the degree of irritation required. A mustard leaf or plaster should not be left on longer than ten or fifteen minutes, unless it is desired to produce a blister. Blistering may be produced by a cantharides plaster, or by painting with liquor epispasticus. The plaster should be left on from eight to ten hours, and if it has failed to raise a blister, a hot fomentation should be applied to the part. Liquor epispasticus, alone or mixed with equal parts of collodion, is painted on the part with a brush. Several paintings are often required before a blister is raised. The preliminary removal of the natural grease from the skin favours the action of these applications.
The treatment of inflammation in special tissues and organs will be considered in the sections devoted to regional surgery.
Chronic Inflammation.—A variety of types of chronic and subacute inflammation are met with which, owing to ignorance of their causations, cannot at present be satisfactorily classified.
The best defined group is that of the granulomata, which includes such important diseases as tuberculosis and syphilis, and in which different types of chronic inflammation are caused by infection with a specific organism, all having the common character, however, that abundant granulation tissue is formed in which cellular changes are more in evidence than changes in the blood vessels, and in which the subsequent degeneration and necrosis of the granulation tissue results in the breaking down and destruction of the tissue in which it is formed. Another group is that in which chronic inflammation is due to mild or attenuated forms of pyogenic infection affecting especially the lymph glands and the bone marrow. In the glands of the groin, for example, associated with various forms of irritation about the external genitals, different types of chronic lymphadenitis are met with; they do not frankly suppurate as do the acute types, but are attended with a hyperplasia of the tissue elements which results in enlargement of the affected glands of a persistent, and sometimes of a relapsing character. Similar varieties of osteomyelitis are met with that do not, like the acute forms, go on to suppuration or to death of bone, but result in thickening of the bone affected, both on the surface and in the interior, resulting in obliteration of the medullary canal.
A third group of chronic inflammations are those that begin as an acute pyogenic inflammation, which, instead of resolving completely, persists in a chronic form. It does so apparently because there is some factor aiding the organisms and handicapping the tissues, such as the presence of a foreign body, a piece of glass or metal, or a piece of dead bone; in these circumstances the inflammation persists in a chronic form, attended with the formation of fibrous tissue, and, in the case of bone, with the formation of new bone in excess. It will be evident that in this group, chronic inflammation and repair are practically interchangeable terms.
There are other groups of chronic inflammation, the origin of which continues to be the subject of controversy. Reference is here made to the chronic inflammations of the synovial membrane of joints, of tendon sheaths and of bursæ—chronic synovitis, teno-synovitis and bursitis; of the fibrous tissues of joints—chronic forms of arthritis; of the blood vessels—chronic forms of endarteritis and of phlebitis and of the peripheral nerves—neuritis. Also in the breast and in the prostate, with the waning of sexual life there may occur a formation of fibrous tissue—chronic interstitial mastitis, chronic prostatitis, having analogies with the chronic interstitial inflammations of internal organs like the kidney—chronic interstitial nephritis; and in the breast and prostate, as in the kidney, the formation of fibrous tissue leads to changes in the secreting epithelium resulting in the formation of cysts.
Lastly, there are still other types of chronic inflammation attended with the formation of fibrous tissue on such a liberal scale as to suggest analogies with new growths. The best known of these are the systematic forms of fibromatosis met with in the central nervous system and in the peripheral nerves—neuro-fibromatosis; in the submucous coat of the stomach—gastric fibromatosis; and in the colon—intestinal fibromatosis.
These conditions will be described with the tissues and organs in which they occur.
In the treatment of chronic inflammations, pending further knowledge as to their causation, and beyond such obvious indications as to help the tissues by removing a foreign body or a piece of dead bone, there are employed—empirically—a number of procedures such as the induction of hyperæmia, exposure to the X-rays, and the employment of blisters, cauteries, and setons. Vaccines may be had recourse to in those of bacterial origin.