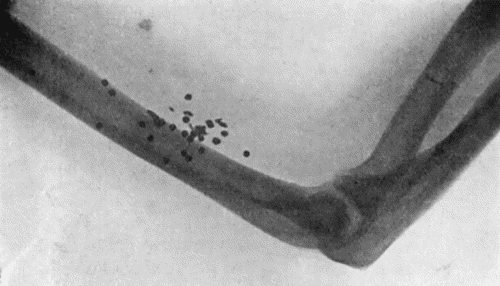
Fig. 62.—Radiogram showing Pellets embedded in Arm.
(Mr. J. W. Dowden's case.)
It is not necessary here to do more than indicate the general characters of wounds produced by modern weapons. For further details the reader is referred to works on military surgery. Experience has shown that the nature and severity of the injuries sustained in warfare vary widely in different campaigns, and even in different fields of the same campaign. Slight variations in the size, shape, and weight of rifle bullets, for example, may profoundly modify the lesions they produce: witness the destructive effect of the pointed bullet compared with that of the conical form previously used. The conditions under which the fighting is carried on also influence the wounds. Those sustained in the open, long-range fighting of the South African campaign of 1899–1902 were very different from those met with in the entrenched warfare in France in 1914–1918. It has been found also that the infective complications are greatly influenced by the terrain in which the fighting takes place. In the dry, sandy, uncultivated veldt of South Africa, bullet wounds seldom became infected, while those sustained in the highly manured fields of Belgium were almost invariably contaminated with putrefactive organisms, and gaseous gangrene and tetanus were common complications. It has been found also that wounds inflicted in naval engagements present different characters from those sustained on land. Many other factors, such as the physical and mental condition of the men, the facilities for affording first aid, and the transport arrangements, also play a part in determining the nature and condition of the wounds that have to be dealt with by military surgeons.
Whatever the nature of the weapon concerned, the wound is of the punctured, contused, and lacerated variety. Its severity depends on the size, shape, and velocity of the missile, the range at which the weapon is discharged, and the part of the body struck.
Shock is a prominent feature, but its degree, as well as the time of its onset, varies with the extent and seat of the injury, and with the mental state of the patient when wounded. We have observed pronounced shock in children after being shot even when no serious injury was sustained. At the moment of injury the patient experiences a sensation which is variously described as being like the lash of a whip, a blow with a stick, or an electric shock. There is not much pain at first, but later it may become severe, and is usually associated with intense thirst, especially when much blood has been lost.
In all forms of wounds sustained in warfare, septic infection constitutes the main risk, particularly that resulting from streptococci. The presence of anaërobic organisms introduces the additional danger of gaseous forms of gangrene.
The earlier the wound is disinfected the greater is the possibility of diminishing this risk. If cleansing is carried out within the first six hours the chance of eliminating sepsis is good; with every succeeding six hours it diminishes, until after twenty-four hours it is seldom possible to do more than mitigate sepsis. (J. T. Morrison.)
The presence of a metallic foreign body having been determined and its position localised by means of the X-rays, all devitalised and contaminated tissue is excised, the foreign material, e.g., a missile, fragments of clothing, gravel and blood-clot, removed, the wound purified with antiseptics and closed or drained according to circumstances.
Pistol-shot Wounds.—Wounds inflicted by pistols, revolvers, and small air-guns are of frequent occurrence in civil practice, the weapon being discharged usually by accident, but frequently with suicidal, and sometimes with homicidal intent.
With all calibres and at all ranges, except actual contact, the wound of entrance is smaller than the bullet. If the weapon is discharged within a foot of the body, the skin surrounding the wound is usually stained with powder and burned, and the hair singed. At ranges varying from six inches to thirty feet, grains of powder may be found embedded in the skin or lying loose on the surface, the greater the range the wider being the area of spread. When black powder is used, the embedded grains usually leave a permanent bluish-black tattooing of the skin. When the weapon is placed in contact with the skin, the subcutaneous tissues are lacerated over an area of two or three inches around the opening made by the bullet and smoke and powder-staining and scorching are more marked than at longer ranges.
When the bullet perforates, the exit wound is usually larger and more extensively lacerated than the wound of entrance. Its margins are as a rule everted, and it shows no marks of flame, smoke, or powder. These features are common to all perforations caused by bullets.
Pistol wounds only produce dangerous effects when fired at close range, and when the cavities of the skull, the thorax, or the abdomen are implicated. In the abdomen a lethal injury may readily be caused even by pistols of the “toy” order. These injuries will be described with regional surgery.
Pistol-shot wounds of joints and soft parts are seldom of serious import apart from the risk of hæmorrhage and of infection.
Treatment.—The treatment of wounds of the soft parts consists in purifying the wounds of entrance and exit and the surrounding skin, and in providing for drainage if this is indicated.
There being no urgency for the removal of the bullet, time should be taken to have it localised by the X-rays, preferably by stereoscopic plates. In some cases it is not necessary to remove the bullet.
Wounds by Sporting Guns.—In the common sporting or scatter gun, with which accidents so commonly occur during the shooting season, the charge of small shot or pellets leave the muzzle of the gun as a solid mass which makes a single ragged wound having much the appearance of that caused by a single bullet. At a distance of from four to five feet from the muzzle the pellets begin to disperse so that there are separate punctures around the main central wound. As the range increases, these outlying punctures make a wider and wider pattern, until at a distance of from eighteen to twenty feet from the muzzle, the scattering is complete, there is no longer any central wound, and each individual pellet makes its own puncture. From these elementary data, it is usually possible, from the features of the wound, to arrive at an approximately accurate conclusion regarding the range at which the gun was discharged, and this may have an important bearing on the question of accident, suicide, or murder.
As regards the effects on the tissues at close range, that is, within a few feet, there is widespread laceration and disruption; if a bone is struck it is shattered, and portions of bone may be displaced or even driven out through the exit wound.
When the charge impinges over one of the large cavities of the body, the shot may scatter widely through the contained viscera, and there is often no exit wound. In the thorax, for example, if a rib is struck, the charge and possibly fragments of bone, will penetrate the pleura, and be dispersed throughout the lung; in the head, the skull may be shattered and the brain torn up; and in the abdomen, the hollow viscera may be perforated in many places and the solid organs lacerated.
On covered parts the clothing, by deflecting the shot, influences the size and shape of the wound; the entrance wound is increased in size and more ragged, and portions of the clothes may be driven into the tissues.
A charge of small shot is much more destructive to blood vessels, tendons, and ligaments than a single bullet, which in many cases pushes such structures aside without dividing them. In the abdomen and chest, also, the damage done by a full charge of shot is much more extensive than that inflicted by a single bullet, the deflection of the pellets leading to a greater number of perforations of the intestine and more widespread laceration of solid viscera.
When the charge impinges on one of the extremities at close range, we often have the opportunity of observing that the exit wound is larger, more ragged than that of entrance, and that its edges are everted; the extensive tearing and bruising of all the tissues, including the bones, and the marked tendency to early and progressive septic infection, render amputation compulsory in the majority of such cases.
At a range of from twenty to thirty feet, although the scatter is complete, the pellets are still close together, so that if they encounter the shaft of a long bone, even the femur, they fracture the bone across, often along with some longitudinal splintering.
Individual pellets striking the shafts of long bones become flattened or distorted, and when cancellated bone is struck they become embedded in it (Fig. 62).
The skin, when it is closely peppered with shot, is liable to lose its vitality, and with the addition of a little sepsis, readily necroses and comes away as a slough.
When the shot have diverged so as to strike singly, they seldom do much harm, but fatal damage may be done to the brain or to the aorta, or the eye may be seriously injured by a single pellet.
Small shot fired at longer ranges—over about a hundred and fifty feet—usually go through the skin, but seldom pierce the fascia, and lie embedded in the subcutaneous tissue, from which they can readily be extracted.
The wad of the cartridge behaves erratically: so long as it remains flat it goes off with the rest of the charge, and is often buried in the wound; but if it curls up or turns on its side, it is usually deflected and flies clear of the shot. It may make a separate wound.
Wounds from sporting guns are to be treated on the usual lines, the early efforts being directed to the alleviation of shock and the prevention of septic infection. There is rarely any urgency in the removal of pellets from the tissues.
Wounds by Rifle Bullets.—The vast majority of wounds inflicted by rifle bullets are met with in the field during active warfare, and fall to be treated by military surgeons. They occasionally occur accidentally, however, during range practice for example, and may then come under the notice of the civil surgeon.
It is only necessary here to consider the effects of modern small-bore rifle or machine-gun bullets.
The trajectory is practically flat up to 675 yards. In destructive effect there is not much difference between the various high velocity bullets used in different armies; they will kill up to a distance of two miles. The hard covering is employed to enable the bullet to take the grooves in the rifle, and to prevent it stripping as it passes through the barrel. It also increases the penetrating power of the missile, but diminishes its “stopping” power, unless a vital part or a long bone is struck. By removing the covering from the point of the bullet, as is done in the Dum-Dum bullet, or by splitting the end, the bullet is made to expand or “mushroom” when it strikes the body, and its stopping power is thereby greatly increased, the resulting wound being much more severe. These “soft-nosed” expanding bullets are to be distinguished from “explosive” bullets which contain substances which detonate on impact. High velocity bullets are unlikely to lodge in the body unless spent, or pulled up by a sandbag, or metal buckle on a belt, or a book in the pocket, or the core and the case separating—“stripping” of the bullet. Spent shot may merely cause bruising of the surface, or they may pass through the skin and lodge in the subcutaneous tissue, or may even damage some deeper structure such as a nerve trunk.
A blank cartridge fired at close range may cause a severe wound, and, if charged with black powder, may leave a permanent bluish-black pigmentation of the skin.
The lesions of individual tissues—bones, nerves, blood vessels—are considered with these.
Treatment of Gunshot Wounds under War Conditions.—It is only necessary to indicate briefly the method of dealing with gunshot wounds in warfare as practised in the European War.
1. On the Field.—Hæmorrhage is arrested in the limbs by an improvised tourniquet; in the head by a pad and bandage; in the thorax or abdomen by packing if necessary, but this should be avoided if possible, as it favours septic infection. If a limb is all but detached it should be completely severed. A full dose of morphin is given hypodermically. The ampoule of iodine carried by the wounded man is broken, and its contents are poured over and around the wound, after which the field dressing is applied. In extensive wounds, the “shell-dressing” carried by the stretcher bearers is preferred. All bandages are applied loosely to allow for subsequent swelling. The fragments of fractured bones are immobilised by some form of emergency splint.
2. At the Advanced Dressing Station, after the patient has had a liberal allowance of warm fluid nourishment, such as soup or tea, a full dose of anti-tetanic serum is injected. The tourniquet is removed and the wound inspected. Urgent amputations are performed. Moribund patients are detained lest they die en route.
3. In the Field Ambulance or Casualty Clearing Station further measures are employed for the relief of shock, and urgent operations are performed, such as amputation for gangrene, tracheotomy for dyspnœa, or laparotomy for perforated or lacerated intestine. In the majority of cases the main object is to guard against infection; the skin is disinfected over a wide area and surrounded with towels; damaged tissue, especially muscle, is removed with the knife or scissors, and foreign bodies are extracted. Torn blood vessels, and, if possible, nerves and tendons are repaired. The wound is then partly closed, provision being made for free drainage, or some special method of irrigation, such as that of Carrel, is adopted. Sometimes the wound is treated with bismuth, iodoform, and paraffin paste (B.I.P.P.) and sutured.
4. In the Base Hospital or Hospital Ship various measures may be called for according to the progress of the wound and the condition of the patient.
Shell Wounds and Wounds produced by Explosions.—It is convenient to consider together the effects of the bursting of shells fired from heavy ordnance and those resulting in the course of blasting operations from the discharge of dynamite or other explosives, or from the bursting of steam boilers or pipes, the breaking of machinery, and similar accidents met with in civil practice.
Wounds inflicted by shell fragments and shrapnel bullets tend to be extensive in area, and show great contusion, laceration, and destruction of the tissues. The missiles frequently lodge and carry portions of the clothing and, it may be, articles from the man's pocket, with them. Shell wounds are attended with a considerable degree of shock. On account of the wide area of contusion which surrounds the actual wound produced by shell fragments, amputation, when called for, should be performed some distance above the torn tissues, as there is considerable risk of sloughing of the flaps.
Wounds produced by dynamite explosions and the bursting of boilers have the same general characters as shell wounds. Fragments of stone, coal, or metal may lodge in the tissues, and favour the occurrence of infective complications.
All such injuries are to be treated on the general principles governing contused and lacerated wounds.