Fig. 60.—Carpal Ganglion in a woman æt. 25.
This term is applied to a cyst filled with a clear colourless jelly or colloid material, met with in the vicinity of a joint or tendon sheath.
The commonest variety—the carpal ganglion—popularly known as a sprained sinew—is met with as a smooth, rounded, or oval swelling on the dorsal aspect of the carpus, usually towards its radial side (Fig. 60). It is situated over one of the intercarpal or other joints in this region, and may be connected with one or other of the extensor tendons. The skin and fascia are movable over the cyst. The cyst varies in size from a pea to a pigeon's egg, and usually attains its maximum size within a few months and then remains stationary. It becomes tense and prominent when the hand is flexed towards the palm. Its appearance is usually ascribed to some strain of the wrist—for example, in girls learning gymnastics. It may cause no symptoms or it may interfere with the use of the hand, especially in grasping movements and when the hand is dorsiflexed. In girls it may give rise to pain which shoots up the arm. Ganglia are also met with on the dorsum of the metacarpus and on the palmar aspect of the wrist.
The tarsal ganglion is situated on the dorsum of the foot over one or other of the intertarsal joints. It is usually smaller, flatter, and more tense than that met with over the wrist, so that it is sometimes mistaken for a bony tumour. It rarely causes symptoms, unless so situated as to be pressed upon by the boot.
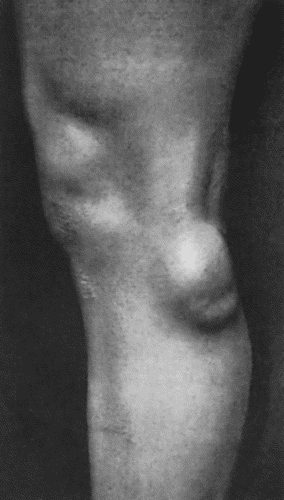
Ganglia in the region of the knee are usually situated over the interval between the femur and tibia, most often on the lateral aspect of the joint in front of the tendon of the biceps (Fig. 61). The swelling, which may attain the size of half a walnut, is tense and hard when the knee is extended, and becomes softer and more prominent when it is flexed. They are met with in young adults who follow laborious occupations or who indulge in athletics, and they cause stiffness, discomfort, and impairment of the use of the limb. A ganglion is sometimes met with on the median aspect of the head of the metatarsal bone of the great toe and may be the cause of considerable suffering; it is indistinguishable from the thickened and enlarged bursa so commonly present in this situation in the condition known as bunion.
Ganglionic cysts are met with in other situations than those mentioned, but they are so rare as not to require separate description.
Ganglia are to be diagnosed by their situation and physical characters; enlarged bursæ, synovial cysts, and new-growths are the swellings most likely to be mistaken for them. The diagnosis is sometimes only cleared up by withdrawing the clear, jelly-like contents through a hollow needle.
Pathological Anatomy.—The wall of the cyst is composed of fibrous tissue closely adherent to or fused with the surrounding tissues, so that it cannot be shelled out. There is no endothelial lining, and the fibrous tissue of the wall is in immediate contact with the colloid material in the interior, which appears to be derived by a process of degeneration from the surrounding connective tissue. In the region of the knee the ganglion is usually multilocular, and consists of a meshwork of fibrous tissue, the meshes of which are occupied by colloid material.
It is often stated that a ganglion originates from a hernial protrusion of the synovial membrane of a joint or tendon sheath. We have not been able to demonstrate any communication between the cavity of the cyst and that of an adjacent tendon sheath or joint. It is possible, however, that the cyst may originate from a minute portion of synovial membrane being protruded and strangulated so that it becomes disconnected from that to which it originally belonged; it may then degenerate and give rise to colloid material, which accumulates and forms a cyst. Ledderhose and others regard ganglia as entirely new formations in the peri-articular tissues, resulting from colloid degeneration of the fibrous tissue of the capsular ligament, occurring at first in numerous small areas which later coalesce. Ganglia are probably, therefore, of the nature of degeneration cysts arising in the capsule of joints, in tendons, and in their sheaths.
Treatment.—A ganglion can usually be got rid of by a modification of the old-fashioned seton. The skin and cyst wall are transfixed by a stout needle carrying a double thread of silkworm gut; some of the colourless jelly escapes from the punctures; the ends of the thread are tied and cut short, and a dressing is applied. A week later the threads are removed and the minute punctures are sealed with collodion. The action of the threads is to convert the cyst wall into granulation tissue, which undergoes the usual conversion into scar tissue. If the cyst re-forms, it should be removed by open dissection under local anæsthesia. Puncture with a tenotomy knife and scraping the interior, and the injection of irritants, are alternative, but less satisfactory, methods of treatment.
Ganglia in the substance of tendons are rare. The diagnosis rests on the observation that the small tumour is cystic, and that it follows the movements of the tendon. The cyst is at first multiple, but the partitions disappear, and the spaces are thrown into one. The tendon is so weakened that it readily ruptures. The best treatment is to resect the affected segment of tendon.
The so-called “compound palmar ganglion” is a tuberculous disease of the tendon sheaths, and is described with diseases of tendon sheaths.