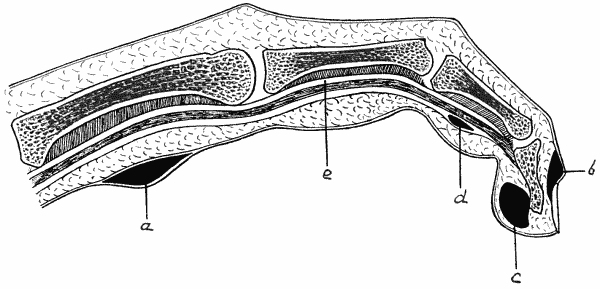
Fig. 9.—Diagram of various forms of Whitlow.
- a = Purulent blister.
- b = Suppuration at nail fold.
- c = Subcutaneous whitlow.
- d = Whitlow in sheath of flexor tendon (e).
The clinical term whitlow is applied to an acute infection, usually followed by suppuration, commonly met with in the fingers, less frequently in the toes. The point of infection is often trivial—a pin-prick, a puncture caused by a splinter of wood, a scratch, or even an imperceptible lesion of the skin.
Several varieties of whitlow are recognised, but while it is convenient to describe them separately, it is to be clearly understood that clinically they merge one into another, and it is not always possible to determine in which connective-tissue plane a given infection has originated.
Initial Stage.—Attention is usually first attracted to the condition by a sensation of tightness in the finger and tenderness when the part is squeezed or knocked against anything. In the course of a few hours the part becomes red and swollen; there is continuous pain, which soon assumes a throbbing character, particularly when the hand is dependent, and may be so severe as to prevent sleep, and the patient may feel generally out of sorts.
If a constricting band is applied at this stage, the infection can usually be checked and the occurrence of suppuration prevented. If this fails, or if the condition is allowed to go untreated, the inflammatory reaction increases and terminates in suppuration, giving rise to one or other of the forms of whitlow to be described.
The Purulent Blister.—In the most superficial variety, pus forms between the rete Malpighii and the stratum corneum of the skin, the latter being raised as a blister in which fluctuation can be detected (Fig. 9, a). This is commonly met with in the palm of the hand of labouring men who have recently resumed work after a spell of idleness. When the blister forms near the tip of the finger, the pus burrows under the nail—which corresponds to the stratum corneum—raising it from its bed.
There is some local heat and discoloration, and considerable pain and tenderness, but little or no constitutional disturbance. Superficial lymphangitis may extend a short distance up the forearm. By clipping away the raised epidermis, and if necessary the nail, the pus is allowed to escape, and healing speedily takes place.
Whitlow at the Nail Fold.—This variety, which is met with among those who handle septic material, occurs in the sulcus between the nail and the skin, and is due to the introduction of infective matter at the root of the nail (Fig. 9, b). A small focus of suppuration forms under the nail, with swelling and redness of the nail fold, causing intense pain and discomfort, interfering with sleep, and producing a constitutional reaction out of all proportion to the local lesion.
To allow the pus to escape, it is necessary, under local anæsthesia, to cut away the nail fold as well as the portion of nail in the infected area, or, it may be, to remove the nail entirely. If only a small opening is made in the nail it is apt to be blocked by granulations.
Fig. 9.—Diagram of various forms of Whitlow.
Subcutaneous Whitlow.—In this variety the infection manifests itself as a cellulitis of the pulp of the finger (Fig. 9, c), which sometimes spreads towards the palm of the hand. The finger becomes red, swollen, and tense; there is severe throbbing pain, which is usually worst at night and prevents sleep, and the part is extremely tender on pressure. When the palm is invaded there may be marked œdema of the back of the hand, the dense integument of the palm preventing the swelling from appearing on the front. The pus may be under such tension that fluctuation cannot be detected. The patient is usually able to flex the finger to a certain extent without increasing the pain—a point which indicates that the tendon sheaths have not been invaded. The suppurative process may, however, spread to the tendon sheaths, or even to the bone. Sometimes the excessive tension and virulent toxins induce actual gangrene of the distal part, or even of the whole finger. There is considerable constitutional disturbance, the temperature often reaching 101° or 102° F.
The treatment consists in applying a constriction band and making an incision over the centre of the most tender area, care being taken to avoid opening the tendon sheath lest the infection be conveyed to it. Moist dressings should be employed while the suppuration lasts. Carbolic fomentations, however, are to be avoided on account of the risk of inducing gangrene.
Whitlow of the Tendon Sheaths.—In this form the main incidence of the infection is on the sheaths of the flexor tendons, but it is not always possible to determine whether it started there or spread thither from the subcutaneous cellular tissue (Fig. 9, d). In some cases both connective tissue planes are involved. The affected finger becomes red, painful, and swollen, the swelling spreading to the dorsum. The involvement of the tendon sheath is usually indicated by the patient being unable to flex the finger, and by the pain being increased when he attempts to do so. On account of the anatomical arrangement of the tendon sheaths, the process may spread into the forearm—directly in the case of the thumb and little finger, and after invading the palm in the case of the other fingers—and there give rise to a diffuse cellulitis which may result in sloughing of fasciæ and tendons. When the infection spreads into the common flexor sheath under the transverse carpal (anterior annular) ligament, it is not uncommon for the intercarpal and wrist joints to become implicated. Impaired movement of tendons and joints is, therefore, a common sequel to this variety of whitlow.
The treatment consists in inducing passive hyperæmia by Bier's method, and, if this is done early, suppuration may be avoided. If pus forms, small incisions are made, under local anæsthesia, to relieve the tension in the sheath and to diminish the risk of the tendons sloughing. No form of drain should be inserted. In the fingers the incisions should be made in the middle line, and in the palm they should be made over the metacarpal bones to avoid the digital vessels and nerves. If pus has spread under the transverse carpal ligament, the incision must be made above the wrist. Passive movements and massage must be commenced as early as possible and be perseveringly employed to diminish the formation of adhesions and resulting stiffness.
Subperiosteal Whitlow.—This form is usually an extension of the subcutaneous or of the thecal variety, but in some cases the inflammation begins in the periosteum—usually of the terminal phalanx. It may lead to necrosis of a portion or even of the entire phalanx. This is usually recognised by the persistence of suppuration long after the acute symptoms have passed off, and by feeling bare bone with the probe. In such cases one or more of the joints are usually implicated also, and lateral mobility and grating may be elicited. Recovery does not take place until the dead bone is removed, and the usefulness of the finger is often seriously impaired by fibrous or bony ankylosis of the interphalangeal joints. This may render amputation advisable when a stiff finger is likely to interfere with the patient's occupation.